Based on the 2020 Medicare Part D plan bids and current Medicare drug plan (PDP and MAPD) enrollment, the 2020 average weighted basic monthly premium is projected to be around $30 per month - a decrease of $2.50 from the $32.50 per month premium projected for 2019 - and down $3.50 from the $33.50 average that was projected for 2018. The 2018 basic premium projection was a $1.20 decrease from the $34.70 actual average premium reported in 2017.
Does the projected decrease in projected average Medicare Part D premiums mean you will pay less for your 2020 Medicare Part D plan?
Not exactly. The average monthly Medicare Part D premium figure released by CMS may not reflect the actual changes you see in your 2020 Medicare Part D prescription drug plan premiums - or overall coverage.
The 2020 average premium of $30 projected by CMS suggests that you should be able to shop around during the annual Open Enrollment Period and find a stand-alone 2020 Medicare prescription drug plan (PDP) with about the same monthly premium as you currently have now, or you may want to consider changing enrollment to a low-premium (or $0 premium) Medicare Advantage plan that includes prescription drug coverage (MAPD).
In addition, our analysis (see below) shows that, although average (unweighted) Medicare Part D plan premiums have been decreasing for the past few years, the average stand-alone Medicare Part D (PDP-only) premium weighted by plan enrollment has been increasing, perhaps indicating that Medicare beneficiaries are choosing Medicare Part D plans with higher premiums or staying with their same plans although their plan premiums have increased.
When can I see the 2020 Medicare Part D and Medicare Advantage plans?
Starting in October, people with Medicare Part D can begin to research their Medicare health and prescription plan options. During the annual Open Enrollment Period (AEP) that begins Tuesday, October 15th and ends Saturday, December 7, 2019, beneficiaries can switch Medicare plans by enrolling in their newly selected plan. If you are not sure where to begin with the annual plan review process, you can start by calling a Medicare representative at 1-800-MEDICARE for more information.
Will my 2019 Medicare Part D plan inform me about 2020 plan changes?
Yes. Everyone with a Medicare Part D or Medicare Advantage plan should review their Medicare plan's Annual Notice of Change letter (ANOC) that will be mailed in late-September or early-October. Even if your Medicare Part D plan premium remains stable (or decrease like the CMS projection) – this does not mean that your 2020 Medicare plan’s drug coverage costs will decrease. Your Medicare drug plan's prescription coverage - which drugs are covered and at what cost - usually changes every year, even if your monthly Medicare plan premium remains the same or decreases slightly.
Finally, Medicare Part D plan members should review their Medicare plan's 2020 Evidence of Coverage (EOC) document mailed to them in early-October - or made available electronically for download. The EOC is a 200+ page document that includes detailed information about the Medicare plan's coverage.
Bottom Line: Medicare Part D plans change each year, so please be prepared to review your 2020 Medicare plan options starting in early October.
How have projected Medicare Part D premiums changed over time?
The following are Medicare's annual projected basic Medicare Part D premiums weighted by enrollment. The actual annual average Medicare Part D premium reported by Medicare may be slightly higher or lower than the projected premium depending on actual Medicare plan enrollment for the year (for example, the actual 2018 average premium was $33.59 as compared to the projected average Part D premium of $33.50).

The projected average basic Medicare Part D premiums reported by CMS include both stand-alone Medicare Part D plans (PDPs) and Medicare Advantage plans that include drug coverage (MAPDs) - and are usually much lower than the actual average Medicare Part D premiums we report each year in our PDP landscape analysis or PDP-Facts section.
The difference between the CMS average premium projection and our analysis is because we only consider stand-alone Medicare Part D prescription drug plans (PDPs) in our premium calculations (or calculations showing average premiums weighted by plan enrollment). Unlike CMS, we do not include the premiums for Medicare Advantage plans offering prescription drug coverage (MAPDs) with stand-alone Medicare Part D plans (PDPs) for several reasons:
-
First, Medicare Part D plans (PDPs) are offered on a statewide (or multi-state regional) basis and Medicare Advantage prescription drug plans (MAPDs) are offered within much smaller service areas (ZIP code, partial-ZIP, or county basis) - and more MAPDs are available in densely populated areas where Medicare plans can easily establish healthcare networks as compared to rural areas. So low-premium MAPDs may not be widely available to all Medicare beneficiaries in a state. (As a note, in Alaska, there are no Medicare Advantage plans (MA or MAPD) available anywhere in the state - except those offered in a small area by employer plans).
- In addition, many popular MAPDs have a low or $0 premium and these low premiums tend to skew the average weighted monthly premium for prescription drug coverage toward lower values that are not reflective of the stand-alone Medicare Part D plan (PDP) landscape. In short, a national average of combined PDP and MAPD premiums weighted by enrollment may not reflect the actual stand-alone Medicare Part D plan premiums available to all seniors.
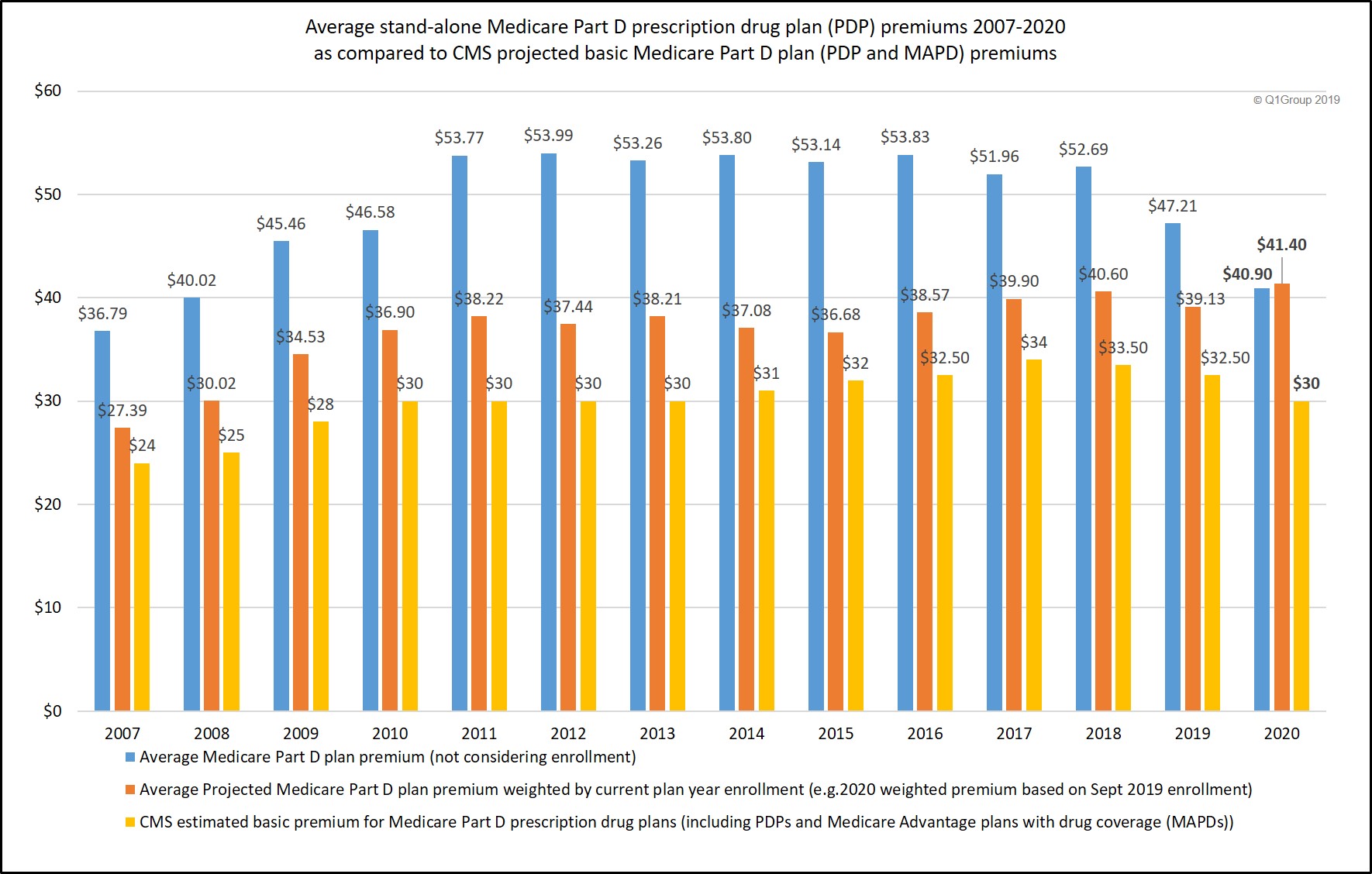
The following chart shows variations or trends in CMS projected basic Medicare Part D plan premiums (PDP and MAPD) as compared to our calculated average stand-alone Medicare Part D plan (PDP-only) premiums and stand-alone Medicare Part D plan (PDP-only) premiums weighted by plan enrollment.
Findings: Over the past few years, average Medicare Part D premiums are decreasing, but since 2015, average PDP premiums weighted by plan enrollment are actually increasing.
From 2015 through 2019, we are seeing an increase in actual average stand-alone Medicare Part D (PDP) premiums weighted by plan enrollment (even though projected and average Medicare Part D premiums have been decreasing over the past few years) - and this increase in weighted premiums may indicate people are either choosing more expensive stand-alone Medicare Part D plans with additional coverage benefits (such as more generous formularies or formulary structures favoring fixed co-pays for popular drugs instead of co-insurance based on ever-changing retail drug prices) - or perhaps people are seeking stability and staying with their same Medicare Part D plans even when their premiums increase and lower-premium plan alternatives are available. Again, our average premiums are for PDPs only - we are not considering any Medicare Advantage plans (MAPDs) that may include low-costing or $0 premium MAPDs.
Here is a summary of our average-weighted PDP premiums over the past years:
- We calculated the 2020 average monthly premium across all
stand-alone Medicare Part D plans (not considering Medicare Advantage
plans offering prescription drug coverage or MAPDs) to be $40.90 - or $41.40 when weighted by stand-alone Medicare Part D plan enrollment. (updated 09/26/2019)
- We calculated the 2019 average monthly premium across all stand-alone Medicare Part D plans (not considering Medicare Advantage plans offering prescription drug coverage or MAPDs) to be $47.21 - or $41.29 when weighted by stand-alone Medicare Part D plan enrollment. (updated 08/04/2019)
- We calculated the 2018 average monthly premium across all
stand-alone Medicare Part D plans (not considering Medicare Advantage
plans offering prescription drug coverage or MAPDs) to be $52.69 - or $43.69
when weighted by stand-alone Medicare Part D plan enrollment. Please
note that "enrollment weighting" can change throughout the plan year as
Medicare plans are sanctioned (and plan members leave the plan) or CMS
lifts Medicare plan sanctions and the plan resumes enrollment or plan
members use a Special Enrollment Period (SEP) to change Medicare plans mid-year. (updated 09/29/2017)
- We calculated the 2017 average monthly premium across all
stand-alone Medicare Part D plans (not considering Medicare Advantage
plans offering prescription drug coverage or MAPDs) to be $51.96 or $42.70
when weighted by stand-alone Medicare Part D plan enrollment.
Please note that "enrollment weighting" can change throughout the plan
year as Medicare plans are sanctioned or removed from sanctions.
(updated 08/02/2017)
- We calculated the 2016 average monthly premium across all stand-alone Medicare Part D plans (not considering Medicare Advantage plans offering prescription drug coverage or MAPDs) to be $53.83 or $39.08 when weighted by stand-alone Medicare Part D plan enrollment (note: the "enrollment weighting" can change throughout the plan year as Medicare plans are sanctioned or removed from sanctions).
- We calculated the 2015 average monthly premium across all stand-alone Medicare Part D plans (not considering Medicare Advantage plans offering prescription drug coverage or MAPDs) to be $53.14 or $36.75 when weighted by stand-alone Medicare Part D plan enrollment.
- We calculated the 2014 average monthly premium across all stand-alone Medicare Part D plans (not considering Medicare Advantage plans offering prescription drug coverage or MAPDs) to be $53.80 or $41.23 when weighted by stand-alone Medicare Part D plan enrollment.
- We calculated the 2013 average monthly premium across all stand-alone Medicare Part D plans to be $53.26 or $40.63 when weighted by all stand-alone Medicare Part D plan enrollment.
- We calculated the 2012 average premium across all stand-alone Medicare Part D plans to be $53.99 or $39.62 when weighted by plan enrollment.
- In 2011, we calculated the average monthly premium across all stand-alone Medicare Part D plans as $53.77 -- or $41.05 when weighted by Medicare Part D plan enrollment.
The full text of the July 30, 2019 CMS Press Release is included below:
Trump Administration Drives Down Drug Costs for Seniors
Today, the Centers for Medicare & Medicaid Services (CMS), under the leadership of President Trump, announced that, for the third year in a row, the average basic premium for Medicare Part D prescription drug plans, which cover prescription drugs that beneficiaries pick up at a pharmacy, is projected to decline. Over the past three years, average Part D basic premiums have decreased by 13.5 percent, from $34.70 in 2017 to a projected $30 in 2020, saving beneficiaries about $1.9 billion in premium costs over that time. As a result, Part D continues to be an extremely popular program, with enrollment increasing 12.2 percent since 2017.
In addition to the premium savings for beneficiaries realized as a result of the increased competition and strengthened negotiations in Part D, the continued decline in Part D bid amounts over the past three years is estimated to save taxpayers nearly $6 billion in the form of lower Medicare premium subsidies.
“President Trump has listened to what American patients and seniors want, and he has promised to protect what works and fix what’s broken in American healthcare,” said HHS Secretary Alex Azar. “Medicare Part D plans continue to be extremely popular, and the President is delivering improvements to Part D, offering plans more ways to provide low-cost options and delivering patients more transparency on drug prices. With premiums in Part D now projected to decline for 2020, President Trump is delivering on his promise to protect seniors and put patients in control.”
“Under President Trump’s leadership, CMS has been taking action to lower the cost of prescription drugs, and we are seeing the results of our actions” said CMS Administrator Seema Verma. “At a time when healthcare costs are going up, the Trump Administration is delivering lower costs to seniors. Part D plans are having to prove their value to beneficiaries – the actions that CMS has taken to strengthen the Medicare prescription drug program are working to drive down costs for seniors.”
In Medicare Part D, beneficiaries choose the prescription drug plan that best meets their needs, and plans have to improve quality and lower costs to attract beneficiaries. This competitive dynamic sets up clear incentives that drive towards value. CMS has taken steps to modernize the Part D program by providing beneficiaries the opportunity to choose among plans with greater negotiating tools that have been developed in the private market and by providing patients with more transparency on drug prices. Increasing competition and strengthening negotiations are key pillars of President Trump’s Blueprint to reduce prescription drug prices, and CMS will continue to implement the President’s Blueprint to ensure that American seniors can access the prescription drugs they need at an affordable price.
Improvements to the Medicare Part D program that CMS has made to date include:
- Providing more information on out-of-pocket
costs for prescription drugs to beneficiaries by requiring Part D plans
to adopt tools that provide clinicians with information that they can
discuss with patients on out-of-pocket drug costs at the time a
prescription is written.
- Implementing Part D legislation signed by
President Trump to prohibit “gag clauses,” which keep pharmacists from
telling patients about lower-cost ways to obtain prescription drugs.
- Requiring the Explanation of Benefits document
that Part D beneficiaries receive each month to include information on
drug price increases and lower-cost therapeutic alternatives.
- Providing beneficiaries with more drug choices
and empowering beneficiaries to select a plan that meets their needs by
allowing plans to cover different prescription drugs for different
indications, an approach used in the private sector.
- Reducing the maximum amount that low-income
beneficiaries pay for certain innovative medicines known as
“biosimilars,” which will lower the cost of these innovative medicines
for these beneficiaries.
- Allowing certain generic drugs to be substituted
onto plan formularies more quickly during the year, so beneficiaries
immediately have lower cost sharing for these drugs.
- Increasing competition among plans by removing the requirement that certain Part D plans have to “meaningfully differ” from each other, making more plan options available for beneficiaries.
The upcoming annual Medicare Open Enrollment period for 2020 begins on October 15, 2019, and ends on December 7, 2019. During this time, Medicare beneficiaries can choose health and drug plans for 2020 by comparing their current coverage and plan quality ratings to other plan offerings, or they can choose to remain in traditional Medicare. For the first time in ten years, the agency is redesigning Medicare Plan Finder, the website for Medicare plan selection, so beneficiaries will be able to more easily compare options and choose the plan that best meets their needs. CMS anticipates releasing the premiums and costs for specific Medicare health and drug plans for the 2020 calendar year in mid-to-late September.
<>To view the 2020 Part D base beneficiary premium, the Part D national average monthly bid amount, the Part D regional low-income premium subsidy amounts, the de minimis amount, the Medicare Advantage employer group waiver plan regional payment rates, and the Medicare Advantage regional PPO benchmarks, visit: and select “2020.”###
Contact: CMS Media Relations press@cms.hhs.gov[Emphasis and Highlighting added]
- 2024 PY CMS Press Release: Q1News.com/1007
- 2023 PY CMS Press Release: Q1News.com/981
- 2022 PY CMS Press Release: Q1News.com/887
- 2021 PY CMS Press Release: Q1News.com/833
- 2020 PY CMS Press Release: Q1News.com/780
- 2019 PY CMS Press Release: Q1News.com/718
- 2018 PY CMS Press Release: Q1News.com/639
- 2017 PY CMS Press Release: Q1News.com/581
- 2016 PY CMS Press Release: Q1News.com/481
- 2015 PY CMS Press Release: Q1News.com/360
- 2014 PY CMS Press Release: Q1News.com/300
- 2013 PY CMS Press Release: Q1News.com/224
- 2012 PY CMS Press Release: Q1News.com/163
- 2011 PY CMS Press Release: Q1News.com/149
- 2010 PY CMS Press Release: Q1News.com/131
- 2009 PY CMS Press Release: Q1News.com/93
- 2008 PY CMS Press Release: Q1News.com/34
- 2007 PY CMS Press Release: Q1News.com/164
8am to 5pm MST
- Sign-up for our Medicare Part D Newsletter.
- PDP-Facts: 2024 Medicare Part D plan Facts & Figures
- 2024 PDP-Finder: Medicare Part D (Drug Only) Plan Finder
- PDP-Compare: 2023/2024 Medicare Part D plan changes
- 2024 MA-Finder: Medicare Advantage Plan Finder
- MA plan changes 2023 to 2024
- Drug Finder: 2024 Medicare Part D drug search
- Formulary Browser: View any 2024 Medicare plan's drug list
- 2024 Browse Drugs By Letter
- Guide to 2023/2024 Mailings from CMS, Social Security and Plans
- Out-of-Pocket Cost Calculator
- Q1Medicare FAQs: Most Read and Newest Questions & Answers
- Q1Medicare News: Latest Articles
- 2025 Medicare Part D Reminder Service