As a reminder: The average monthly Medicare Part D premium figure released by CMS may not reflect the actual changes in your 2017 Medicare Part D prescription drug plan premiums - or overall coverage. Instead, everyone with a Medicare Part D or Medicare Advantage plan should be prepared to research other, more economic forms of health and prescription coverage during the annual Open Enrollment Period that begins Saturday, October 15, 2016 and continues through Wednesday, December 7th.
As reference, here are the weighted average monthly premiums for a standard or basic Medicare Part D prescription drug plan reported by HHS or CMS since 2007 (with links to past blogs). (We do not have a base premium figure from 2005 reporting on the beginning of the Medicare Part D program in 2006).
|
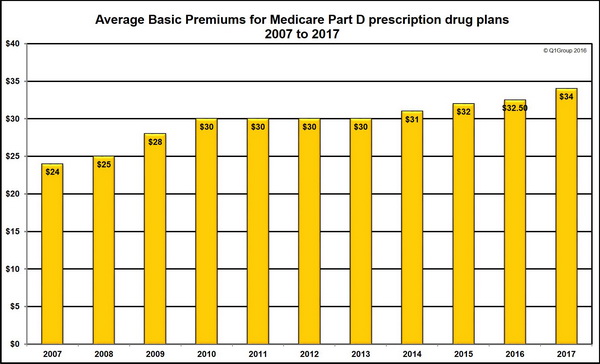
Annual estimated basic Medicare Part D premiums 2007 to 2017
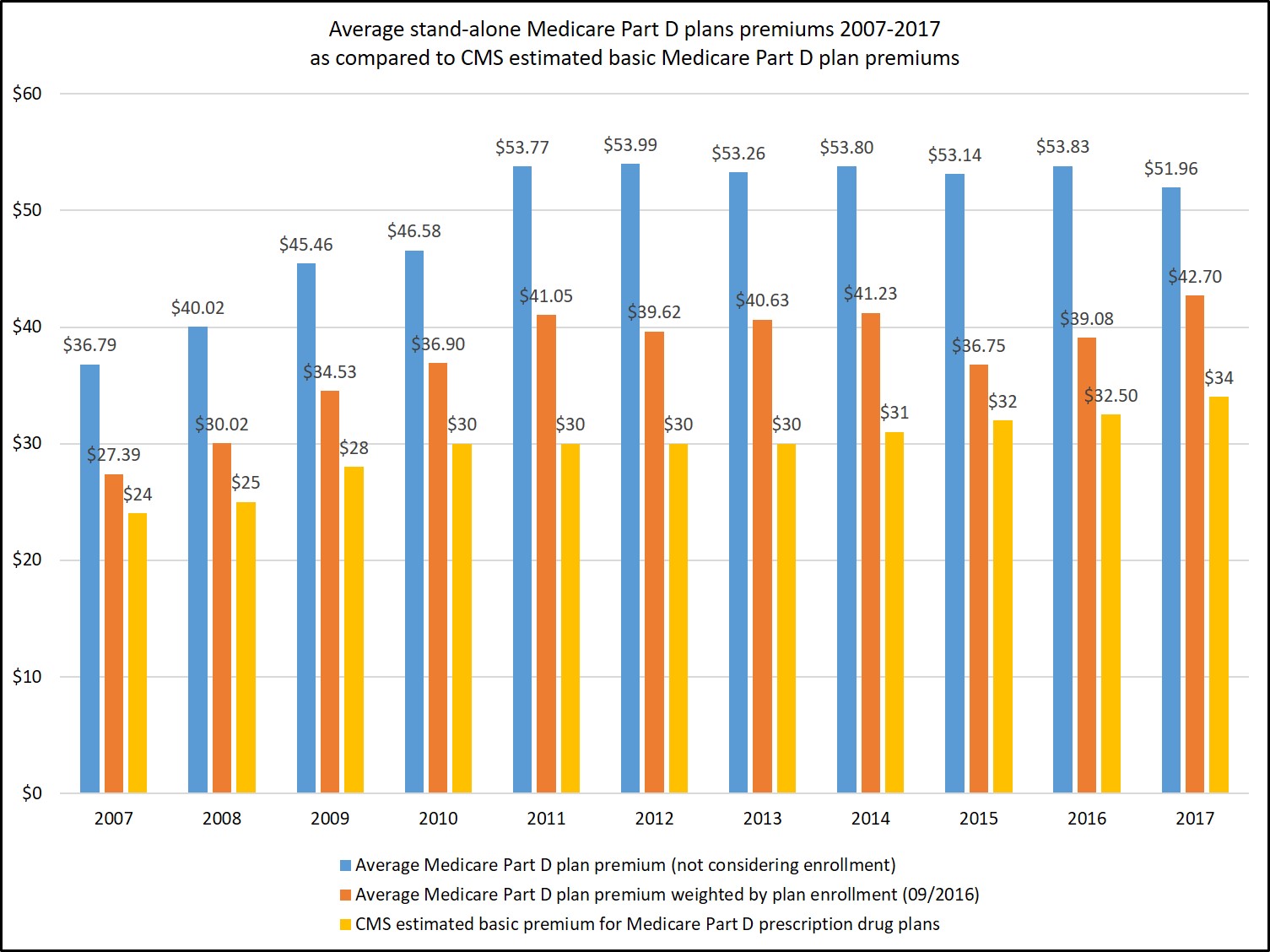
Estimated average basic premiums vs. Actual weighted (and unweighted) stand-alone Medicare Part D premiums from 2007 to 2017
First, Medicare Part D plans are offered on a state-wide (or regional) basis and Medicare Advantage plans are offered within much smaller service areas (ZIP Code or county basis), so Medicare Advantage plans may not be widely available to all Medicare beneficiaries in a state (or in the case of Alaska, there are no Medicare Advantage plans available).
Also, we find that the many of MAPDs have a low or $0 premium and these low premiums tend to skew the average monthly premium for prescription drug coverage toward lower values that are not reflective of the stand-alone Medicare Part D plan (PDP) landscape. At any rate, here are our calculations of average Medicare Part D plan premiums from the past several years along with a chart showing the variation with CMS estimated premium figures:
- We calculated the 2016 average monthly premium across
all stand-alone Medicare Part D plans (not considering Medicare
Advantage plans offering prescription drug coverage or MAPDs) to be $53.83 or $39.08
when weighted by stand-alone Medicare Part D plan enrollment
(note: the "enrollment weighting" can change throughout the plan
year as Medicare plans are sanctioned or removed from sanctions).
- We calculated the 2015 average monthly premium across
all stand-alone Medicare Part D plans (not considering Medicare
Advantage plans offering prescription drug coverage or MAPDs) to be $53.14 or $36.75 when weighted by stand-alone Medicare Part D plan enrollment.
- We calculated the 2014 average monthly premium across
all stand-alone Medicare Part D plans (not considering Medicare
Advantage plans offering prescription drug coverage or MAPDs) to be $53.80 or $41.23 when weighted by stand-alone Medicare Part D plan enrollment.
- We calculated the 2013 average monthly premium across all stand-alone Medicare Part D plans to be $53.26 or $40.63 when weighted by all stand-alone Medicare Part D plan enrollment.
- We calculated the 2012 average premium across all stand-alone Medicare Part D plans to be $53.99 or $39.62 when weighted by plan enrollment.
- In 2011, we calculated the average monthly premium across all stand-alone Medicare Part D plans as $53.77 -- or $41.05 when weighted by Medicare Part D plan enrollment.
No. The 2017 average premium reported by CMS suggests that you should be able to shop around and find a 2017 Medicare prescription drug plan with about the same monthly premium as you currently have now, or you may want to consider changing enrollment to a Medicare Advantage plan that includes prescription drug coverage.
Key Point: Even if your Medicare Part D plan premium remains stable – this does not mean that your 2017 plan’s drug coverage will not change. Your Medicare drug plan's prescription coverage (which drugs are covered and at what cost) can change every year, even if your monthly Medicare plan premium remains the same. So be prepared to review your 2017 Medicare plan options starting in early October 2016.
The full text of the July 29, 2016 CMS Press Release is included below:
Medicare projects relatively stable average prescription drug premiums in 2017
Today, Medicare announced that the average basic premium for a Medicare Part D prescription drug plan in 2017 is projected to remain relatively stable at an estimated $34 per month. This represents an increase of approximately $1.50 over the actual average premium of $32.56 in 2016.
“Stable Medicare prescription drug plan premiums help seniors and people with disabilities afford their prescription drugs,” said Andy Slavitt, Acting Administrator of the Centers for Medicare & Medicaid Services (CMS). “However, I remain increasingly concerned about the rising cost of drugs, especially high-cost specialty drugs, and the impact of these costs on the Medicare program.”
The stability in average basic Medicare Part D premiums for enrollees comes despite the fact that Part D costs continue to increase faster than other parts of Medicare, largely driven by high-cost specialty drugs and their effect on spending in the catastrophic benefit phase. Although private prescription drug plans receive capitated payments for portions of the Part D benefit, Medicare is directly responsible for 80 percent of the cost of drugs purchased by beneficiaries while in the catastrophic benefit phase.
As the recent 2016 Medicare Trustees report noted, growth in the costs of prescription drugs paid by Medicare continue to exceed growth in other Medicare costs and overall health expenditures. Medicare Part D expenditures per enrollee are estimated to increase by an average of 5.8 percent annually through 2025, higher than the combined per-enrollee growth rate for Medicare Parts A and B (4.0 percent). The report found that these costs are trending higher than previously predicted, particularly for specialty drugs. In addition, a March 2016 Department of Health and Human Services report provided a detailed analysis of high-cost prescription drug spending trends.
Today’s projection for the average premium for 2017 is based on bids submitted by drug and health plans for basic drug coverage for the 2017 benefit year and calculated by the independent CMS Office of the Actuary.
Seniors and people with disabilities are continuing to see savings on out of pocket drug costs as the Affordable Care Act closes the Medicare Part D “donut hole” over time. Since the enactment of the Affordable Care Act, more than 10.7 million seniors and people with disabilities have received discounts of over $20.8 billion on prescription drugs, an average of $1,945 per beneficiary.
The upcoming annual Medicare open enrollment period begins on October 15, 2016, and ends on December 7, 2016. During this time, people with Medicare can choose health and drug plans for 2017 by comparing their current coverage and plan quality ratings to other plan offerings, or choose to remain in Original Medicare. CMS anticipates releasing the premiums and costs for Medicare health and drug plans for the 2017 calendar year in mid-September.
To view the Part D Base Beneficiary Premium, the Part D National Average Monthly Bid Amount, the Part D Regional Low-Income Premium Subsidy Amounts, the De Minimis Amount, the Part D Income-Related Monthly Adjustment Amounts, the 2017 Medicare Advantage Employer Group Waiver Plan Regional Payment Rates, and the Medicare Advantage Regional Benchmarks, go to: www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats/Ratebooks-and-Supporting-Data.html, and select “2017.”
To learn more about the Medicare Part D prescription drug benefit, go to: www.medicare.gov/part-d/.
###
Contact: CMS Media Relations
(202) 690-6145 | CMS Media Inquiries
[Emphasis and Highlighting added]
As reference, the text of the July 29, 2015, CMS Press Release "Medicare prescription drug premiums projected to remain stable" can be found at:
- 2024 PY CMS Press Release: Q1News.com/1007
- 2023 PY CMS Press Release: Q1News.com/981
- 2022 PY CMS Press Release: Q1News.com/887
- 2021 PY CMS Press Release: Q1News.com/833
- 2020 PY CMS Press Release: Q1News.com/780
- 2019 PY CMS Press Release: Q1News.com/718
- 2018 PY CMS Press Release: Q1News.com/639
- 2017 PY CMS Press Release: Q1News.com/581
- 2016 PY CMS Press Release: Q1News.com/481
- 2015 PY CMS Press Release: Q1News.com/360
- 2014 PY CMS Press Release: Q1News.com/300
- 2013 PY CMS Press Release: Q1News.com/224
- 2012 PY CMS Press Release: Q1News.com/163
- 2011 PY CMS Press Release: Q1News.com/149
- 2010 PY CMS Press Release: Q1News.com/131
- 2009 PY CMS Press Release: Q1News.com/93
- 2008 PY CMS Press Release: Q1News.com/34
- 2007 PY CMS Press Release: Q1News.com/164
- Sign-up for our Medicare Part D Newsletter.
- PDP-Facts: 2024 Medicare Part D plan Facts & Figures
- 2024 PDP-Finder: Medicare Part D (Drug Only) Plan Finder
- PDP-Compare: 2023/2024 Medicare Part D plan changes
- 2024 MA-Finder: Medicare Advantage Plan Finder
- MA plan changes 2023 to 2024
- Drug Finder: 2024 Medicare Part D drug search
- Formulary Browser: View any 2024 Medicare plan's drug list
- 2024 Browse Drugs By Letter
- Guide to 2023/2024 Mailings from CMS, Social Security and Plans
- Out-of-Pocket Cost Calculator
- Q1Medicare FAQs: Most Read and Newest Questions & Answers
- Q1Medicare News: Latest Articles
- 2025 Medicare Part D Reminder Service